Neuromuscular Care Plan
This is a Summary of your Visit today. Education is provided after the Summary.
DIAGNOSIS:
- Sensory motor polyneuropathy, axonal demyelinating
- Sensory neuropathy
- Small fiber neuropathy
- Myopathy
CAUSE of DIAGNOSIS:
- Diabetes
- Idiopathic
- B12 deficiency
- Thyroid disease
NEEDS ASSESSMENT AND PLAN: During this visit, interventions were prescribed to assist with:
- Nerve Support
- Neuropathic Pain
- Sleep intervention
- Safety
Education
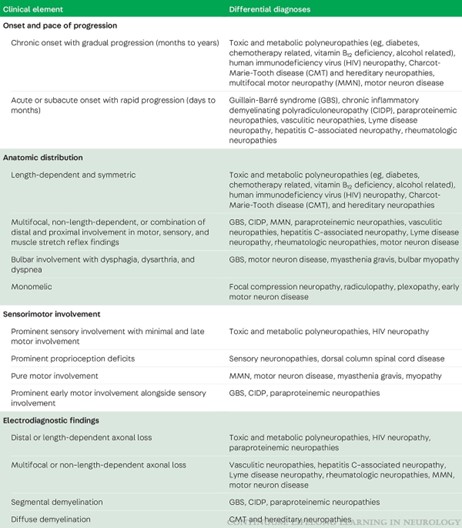
The initial visit seeks to understand the symptoms you are experiencing and beginning to understand how quickly symptoms came on and in what areas. Also what other associated factors may be present that can assist with diagnosis and care.
Common Initial Symptoms of Neuromuscular Conditions:
- Numbness
- Weakness
- Atrophy
- Tingling or Burning
- Gait imbalance
Information Gathered:
- Onset: gradual onset over months to years versus more rapid onset over days to months.
- Location of symptoms:
- Length dependant and symmetric
- Only one limb
- Multiple limbs and/or nerves involved
- Associated with swallowing or speech problems
- Sensory and Motor involvement:
- Sensation and weakness
- Only weakness
- Only sensory
- See this link for further information: https://mclarkgaspervic.com/wp-content/uploads/2025/04/hx-neuromuscular.jpg
Examination along with EMG is helpful in further characterizing the problem. Exams can help at first distinguish between problems in the brain or spinal cord (using reflexes and other parts of the exam).
Electromyography or EMG is an extension of information gathering and helps determine:
- Which nerves or muscle are involved, and if there is a pinched nerve in the neck or back
- Whether problems are at end of limbs (distal) or in hips and shoulders (proximal)
- What type of problem is present: is the nerve damaged (axonal) or is the covering of the nerve damaged (demyelinating)
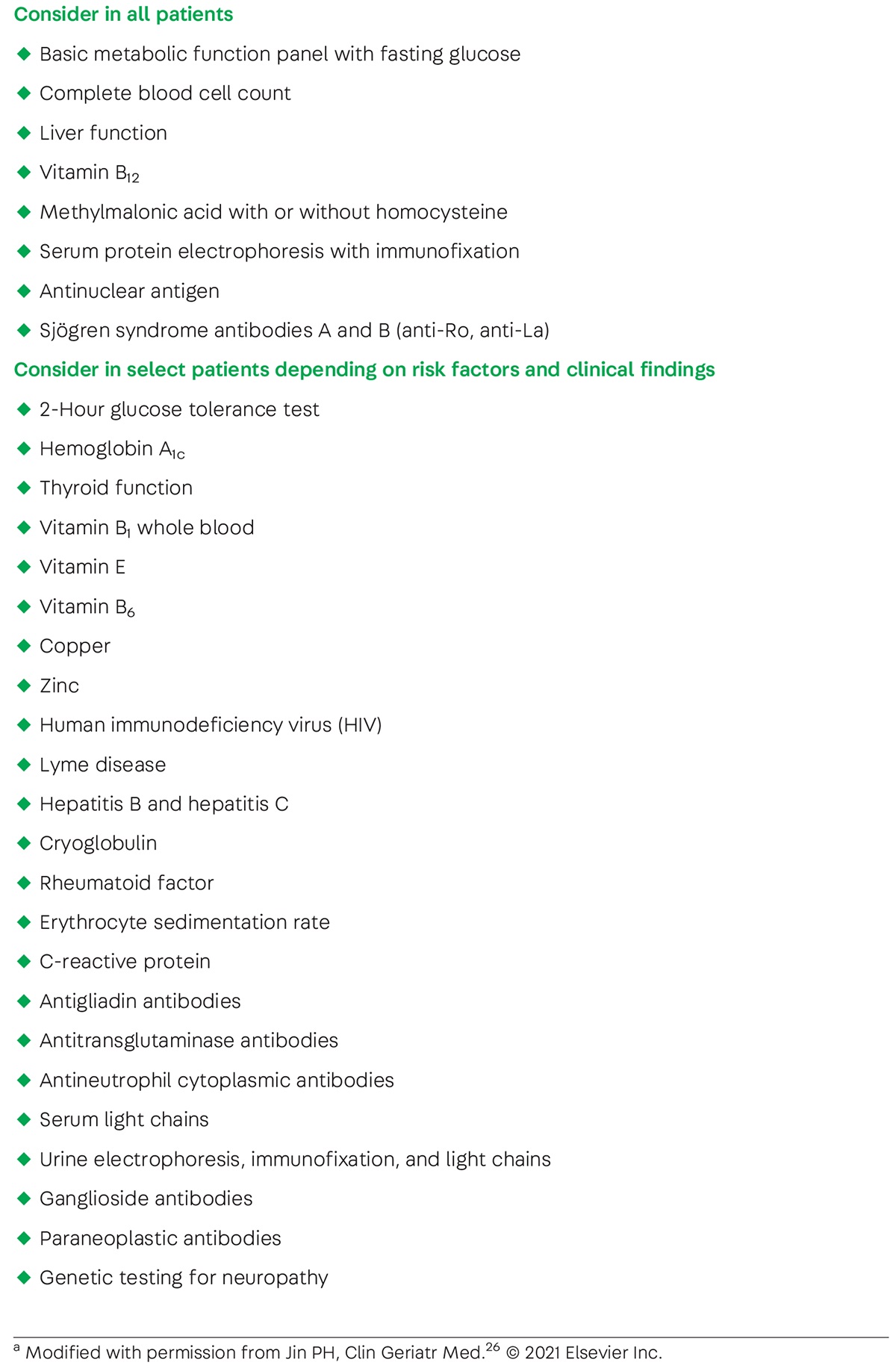
Blood work is helpful in determining why there are problems with the nerves or muscles.
- Table of nerve blood work: https://mclarkgaspervic.com/wp-content/uploads/2025/04/blood-work-neuromuscular.jpeg
Muscle blood worl
Imaging
MRI
Skin Biopsy
Skin biopsy can assist in the evaluation of small fiber neuropathy. Testing is typically pursued in select clinical contexts if evaluation for a polyneuropathy via electrodiagnostic studies is normal. Testing involves a 3-mm punch biopsy of a single limb (generally lower extremity) at sites of interest including the distal leg, distal thigh, and proximal thigh. Biopsy samples are assessed for intraepidermal nerve fiber density, which is expected to be reduced in small fiber neuropathies. The pattern of density loss can also speak to the distal (length-dependent) or multifocal (non–length-dependent) nature of the neuropathy. In addition to intraepidermal nerve fiber density, biopsy samples can be stained to assess for the presence of amyloid deposition and for sudomotor innervation of sweat glands.
Nerve Biopsy
Nerve biopsy is considered in cases of progressive peripheral nerve disease without identified etiology. A sensory nerve is typically selected, most commonly the sural nerve. Nerve biopsy remains most useful in cases of suspected vasculitic neuropathy, neurolymphomatosis, nerve sheath tumors, amyloidosis, sarcoidosis, and leprosy. With these diseases, other diagnostic testing is often insufficient, and specific histopathologic diagnosis can lead to disease-modifying treatment. Beyond these diseases, the utility of nerve biopsy overall is limited. In cases of ambiguous demyelinating and axonal polyneuropathies, histopathology often provides information already retrieved from electrodiagnostic testing
Muscle Biopsy


{kind=link}
{kind=link}